Tendinopathy Pathophysiology
So, if we were to ask what common ailment accounts for 30% of all GP consultations, 30-50% of all sporting injuries, but still occurs in 6% of all sedentary individuals and costs the NHS £250m a year, you’d probably think you’d have heard of it? Tendinopathy, or tendon damage resulting in pain, could be considered an epidemic, but surprisingly it lacks a lot of awareness. I rarely get a patient who has heard of this before (admittedly I do get patients who have heard of ‘tendonitis’, but this is now a redundant term), which as a clinician makes my job harder. As a footnote, you’re more likely to suffer from tendinopathy if you are a smoker, overweight, diabetic, on steroid, statin or flouroquiolone medication, as well as growing older.
So, what is it? Why is it no longer called ‘tendonitis’ and what can osteopathy achieve? You will find out here.
Tendon pathophysiology
Tendons transmit forces from your muscles to your bones, which is fundamental for movement. Because they only transmit the force, they are passive tissues that don’t initiate the movement or force, so they don’t repair themselves in the same way that muscles do.
Tendons don’t like the two C’s –
- Change – a dramatic change in activity levels
- Compression – compression through poor loading/postural positioning (1)
If this happens, they emit very few inflammatory markers, instead hypercellularity happens which is the term we use for an abnormal excess of cells in a particular area. This is why we call it ‘opathy’, meaning disorder, rather than –‘itis’ which means inflammation.
Although we’re not completely sure why it occurs, when tendons degenerate the cell’s function and neovascularisation (formation of new blood vessels) occurs, which is a sign of? tendon pathology.
Below are the three stages of teninopathy:
- Reactive Tendon
- Typically young
- Occurs when loading tendon beyond capacity
- Reversible
- Tendon Disrepair
- Young to middle aged
- In between the two
- Also reversible
- Degenerative Tendon
- Middle age plus
- Further overloaded and damaged, results in tendon thickening
- Irreversible (2)
Tendons require tension
So, the question is what do we do about it? Essentially because tendons require loading to function properly, the answer is further loading, but done properly. Your osteopath or physio with give you a precise exercise program depending on the type of tendinopathy, the health of the surrounding tissues and what you, as an individual, prefer as a training method.
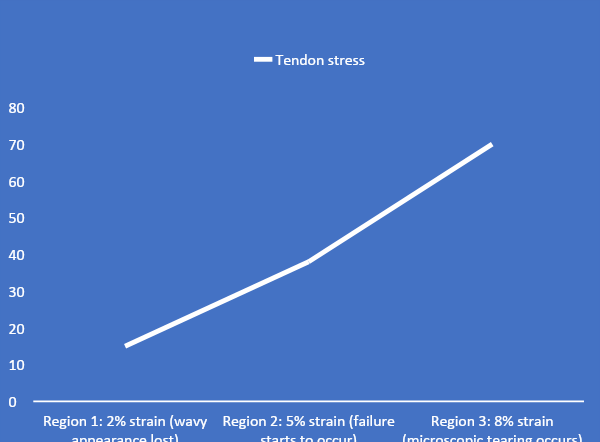
The graph in blue shows how the tendons don’t tolerate much strain – at around 8% strain before microscopic tearing starts to occur. Despite this, studies show achillies tendons can be subjected to 12.5 times your body weight. In an average 50 minute run, the achillies tendon is subjected to 1.68 million Kgs per leg. This may sound high but our tissues are able to deal with the load.
Healthy tendon adaptation occurs when the tendons are put under reasonable stress. In tendons that don’t go through adequate loading, fibrosis starts to occur.
Markers for Improvement
We know that tendons are getting better as they become less painful. There are other measurement tools, the gold standard being ultrasound tissue characterisation, which helps to visualise tendon health.
It is important to know that the prognosis is usually very good, as long as the patient’s compliance is also very good. You want to allocate around 12 weeks for very painful tendons and expect for progress to be very up and down (4).
Lifestyle advice
Lifestyle advice is predicated on the two C’s. Interventions may take the form of suggestions which may include altering training strategies or reducing certain postural dysfunctions. Integrating a good loading program is also vital and the most successful intervention for tendinopathy.
Other risk factors
- Smoking
- Poor diet
- Advancing age
- Medications
- Flouroquiolones (ciprofloxin)
- Steroids
- Statins
- Aromatase inhibitors
- Diabeties (due to glycation of collagen making the tendon more brittle)
- High cholesterol/obesity
- Previous injury/inadequate recovery (5)
For any further questions, please don’t hesitate to ask:
0161 209 2980
info@movementandwellbeingclinic.co.uk
Ed Madeley M.Ost
Referances
- Scott A, Ashe MC Common tendinopathies in the upper and lower extremities. Curr Sports Med Rep. 2006 Sep; 5(5):233-4https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3761855/1.
- Khan K 2007. New Laboratory Insights into the pathogenesis in tendinopathy
- Komi PV1, Fukashiro S, Järvinen M. Biomechanical loading of Achilles tendon during normal locomotion. Clin Sports Med. 1992 Jul;11(3):521-31.
- Kongsgaard M, Qvortrup K, Larsen J, Aagaard P, Doessing S, Hansen P, Kjaer M, Magnusson SP. Fibril morphology and tendon mechanical properties in patellar tendinopathy: effects of heavy slow resistance training. Am J Sports Med. 2010 Apr;38(4):749-56.
- van der Vlist AC1, Breda SJ2, Oei EHG2, Verhaar JAN1, de Vos RJ1. Clinical risk factors for Achilles tendinopathy: a systematic review. Br J Sports Med. 2019 Nov;53(21):1352-1361. doi: 10.1136/bjsports-2018-099991. Epub 2019 Feb 4.