FAI – Femoral Acetabular Impingement
Engaging in sport is fun, healthy and challenging but it can produce injuries. A lot of recreational sporting injuries don’t require a lot of time out and will heal quickly; Femoral Acetabular Impingement (FAI) syndrome typically isn’t one of them.

FAI, a problem concerning the leg bone (femur) and the acetabulum (the socket in the pelvis) is a commonly under diagnosed hip issue. It should be the first thing on the osteopath’s mind when a sporty young patient comes in cupping the the outside of the hip and possibly groin & thigh areas where the pain is. It is typically gradual, activity related pain. The patient will say that it’s worse for pivot type movements, such as turning and cutting in sport, or getting out of a car. FAI is caused by repeated traumatic hip movements during adolescence, which is why it is usually found in young people that engage in sport.
It is an interesting ailment, because although conservative therapy can’t reduce the bony malformation. It can help to reduce the impact between the femur and acetabulum, therefore osteopathy should always be tried before surgery.
What is also interesting about FAI is that just because a scan shows it, you may not have it. The pain reproduced during sporting activities will be the same as that experienced at the osteopath’s clinic during examination.
What are the three types of FAI?
CAM type – Highly provoked through sport participation and the most common type of hip impingement. The head of the femur is more inclined to catch the rim of the hip socket. This causes a natural reaction to such a stimulus called ossification (bone growth)
This is more common in young sporty men and accounts for around 47% of all FAI.
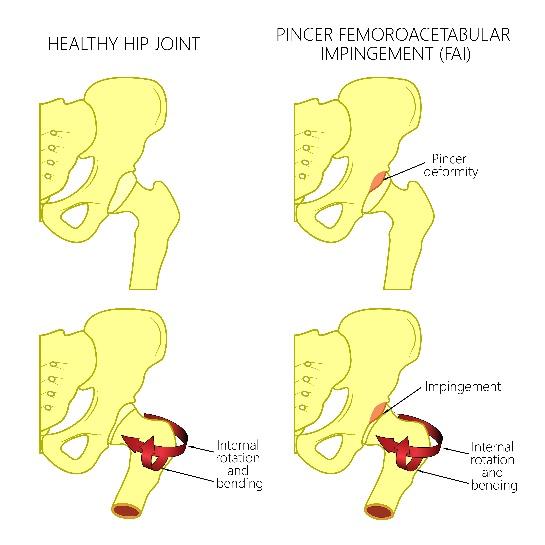
Pincer type – mainly based on an X-ray. What is looked for is acetabulum (the socket of the hip joint) tearing due to a deep or sloped socket, which predisposes FAI. This is more common in middle aged women.
Pincer type occurs in about 8% of all FAI. There are actually two types of pincer:
- Anterior: The anomaly is at the front of the hip; pain is worse when bringing your knee to your opposite shoulder.
- Posterior: The anomaly is at the back of the hip, pain is worse when bringing the leg backwards and out.

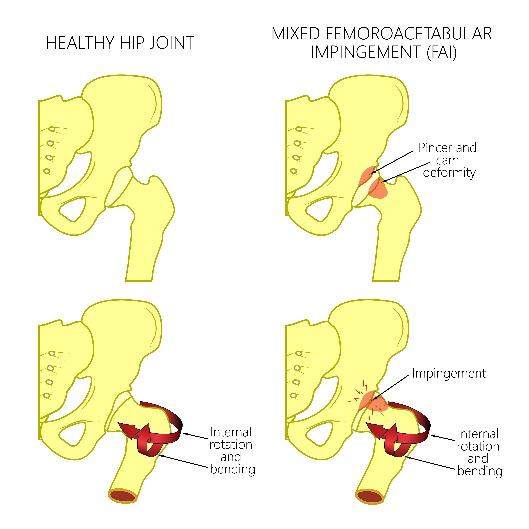
Mixed type – mixed type is a combination of the two.
Studies show that the mixed type is predisposed by your pelvic incidence angle, which is the angle between the line perpendicular to the sacral plate at its midpoint and the line connecting this point to the femoral heads axis.
Leading with lifestyle advice
Although, as osteopaths, we feel that we can heal mainly with our hands, FAI can be treated well with lifestyle advice alongside the hands-on treatment and proper rehab program. The initial assessment is key here, as the type of impingement and reason for the impingement shall dictate the treatment, going forward.
Once the lifestyle advice has been implemented, the hands-on treatment consists of helping to relocate the femoral head from its hazardous position to a more correct one. There are various techniques in the Osteopath’s capabilities that enable this. There is also evidence that shows foot position, standing/sitting posture and thoracic spine mobility play a big part in reducing symptoms of FAI. Again, this will be assessed during your visit to the Movement and Wellbeing Clinic.
For any further questions, please don’t hesitate to ask:
0161 209 2980
info@movementandwellbeingclinic.co.uk
Ed Madeley M.Ost